Understanding how levodopa works in Parkinson's
𝗣𝗮𝗿𝘁 𝟭: 𝗜𝗺𝗺𝗲𝗱𝗶𝗮𝘁𝗲 𝘃𝘀. 𝗟𝗼𝗻𝗴𝘁𝗲𝗿𝗺 𝗘𝗳𝗳𝗲𝗰𝘁𝘀
In response to my advocacy for dopamine reduction therapy, I hear a common response. Levodopa (and other dopaminergic treatments) promptly restoring movement in Parkinson's in almost everyone who receives the treatment argues in support of the disease as being one of dopamine deficiency.
This will be part 1 of the explanation for this paradox between levodopa effects and dopamine excess in Parkinson's, in which I explain how drugs can have different immediate effects than long-term impact.
This is a key point about biology. People and biologic systems often respond to a particular chemical or stimulus differently when first exposed than after chronic exposure. That's me using a bit of jargon to explain that an immediate and a long-term effect of a drug each need to be studied and understood because they are not always the same.
Instead of getting into a bunch of cell and molecular biology, let's consider some examples.
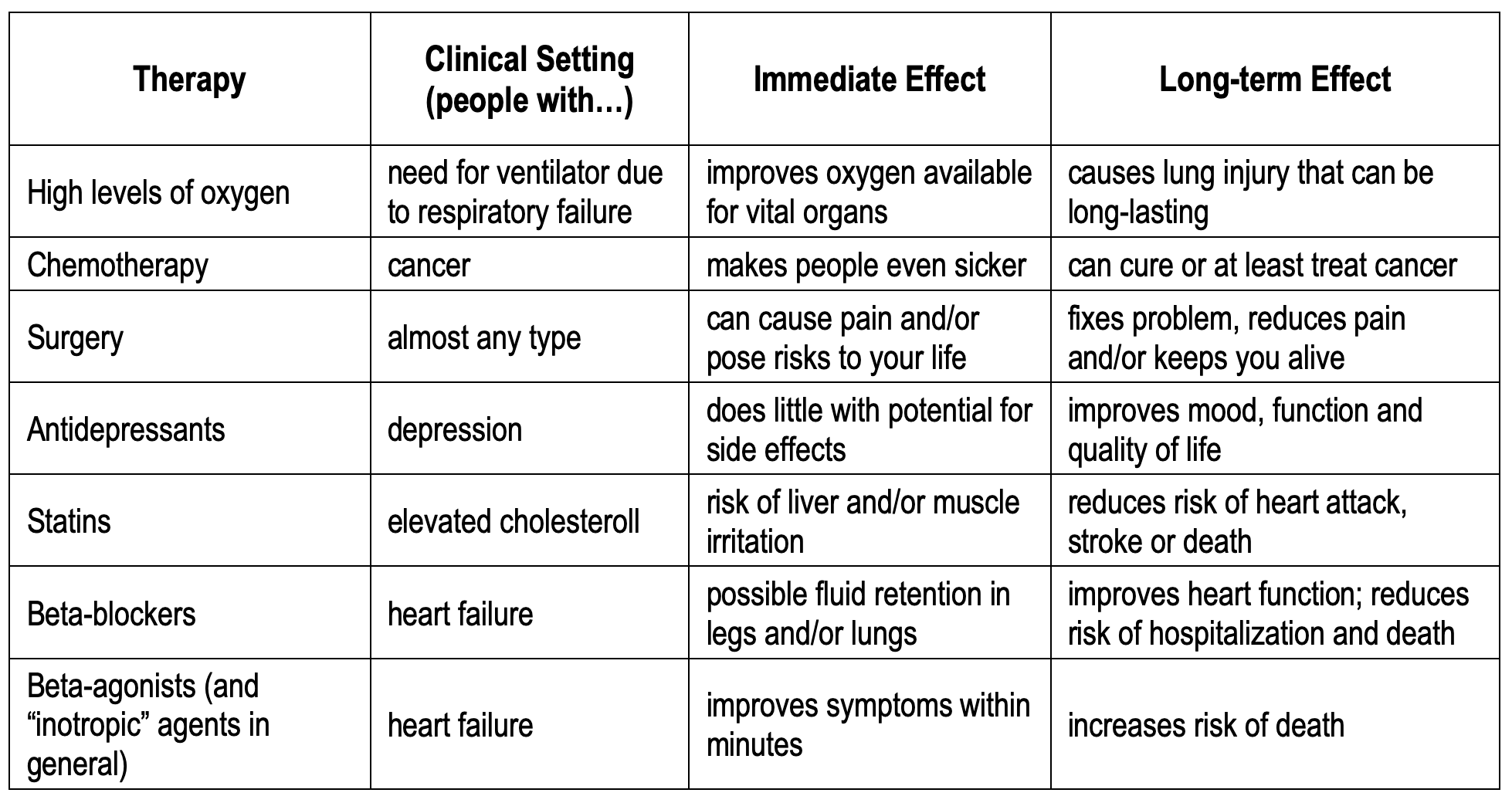
These examples show that the clinical effects of treatments can be different - even opposite - when evaluating in the short-term vs. the long-term. To date, randomized, placebo-controlled trials of levodopa and other dopaminergic therapies have been evaluated rigorously for their immediate and intermediate term effects, not the long-term. But patients know that these drugs don't beat the disease in the long run.
I am not advocating anyone stop dopaminergic therapies. Do I believe the data show that dopaminergic therapies work? Absolutely yes. But the unanswered question is whether dopaminergic therapies are a long-term answer. While some people do experience long-term benefit, many do not. And clinical trials do not show that any of the current drugs slow, stop or reverse disease progression. In fact, clinical trials completed to date have not even evaluated these treatments long-term (longest treatment in placebo controlled trials is ~9-10 months).
So while dopaminergic therapies can be quite useful to manage symptoms of Parkinson's, I believe we'll learn that the best long-term approach is the opposite - dopamine reduction therapy.